Audiological Screening
Screening Principles
Screening programs are used to identify those individuals who have a particular disorder or group of disorders. Screening is warranted when a disorder has appreciable adverse effects on those who have it, and if it can be treated once it has been identified. In addition, the problem should be reasonably widespread in its occurrence, and there must be a test for it that is quick, reliable, and acceptable to those who receive it. These criteria are undeniably met by hearing impairments, disorders, and disabilities, which may be defined as follows (ASHA 1997).1 A disorder is an anatomical abnormality (e.g., an ear deformity) or a pathology (e.g., a middle ear infection). An impairment means that physiological and/or psychological functioning is lost or abnormal (e.g., a hearing loss). A disability occurs when a person’s ability to perform is adversely affected (e.g., when a hearing loss impedes academic performance or social interactions). These areas are addressed by audiological screening programs (AAA 1997a,b; ASHA 1997; NIH 1993; Mauk & Behrens 1993; JCIH 2007). (The term identification audiometry is sometimes used to refer to screening for hearing impairment, and is often encountered in the older literature.)
Hearing screening programs must be supervised by a qualified audiologist, but it is generally agreed that cost-effective mass screening programs entail testing procedures that do not require an audiologist’s expertise (NIH 1993; AAA 1997a,b; ASHA 1997; JCIH 2007). Thus, the goal is for the day-to-day screening activities to be performed by support personnel hired for this purpose, or by non-audiologist professionals who are in the right place at the right time to perform the tests.
1 For consistency, these terms as defined in the ASHA (1997) screening guidelines will be employed throughout this chapter.
Although we will not directly address financial factors in detail here, one must also be aware that the costs of personnel, instrumentation, space, etc., cannot be overlooked, and often play a central role in real-world decisions about screening programs. For these reasons, the clinician may be asked to provide such information as the cost of a screening program on a per-child basis. An example of a typical formula that might be used for this purpose (Copper, Gates, Owen, & Dickson 1975) is
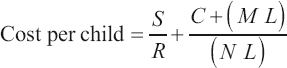
Here, S is the hourly salary of the screening personnel, R is the rate of screening (children tested per hour), C is the cost of the equipment, M is the annual equipment maintenance cost, N is the number of children screened in a year, and L is the expected lifetime (in years) of the equipment.
The fundamental goal of a screening test is to identify the individuals in a population who have a specified disorder or group of disorders. People who actually have the targeted disorder are said to be “abnormal” and those who really do not have that disorder are “normal.” It is important to remember that normality or abnormality here pertains only to the particular disorder(s) being screened. In a perfect screening test every abnormal person would fail and every normal case would pass. In spite of our best intentions, no screening test (or any test, for that matter) can separate all normal and abnormal individuals with complete accuracy. For this reason we must consider the screening process in terms of the percentages of correct and incorrect results. Complicating matters is the issue of what constitutes the “gold standard” used to determine the patient’s “real status.” This is often established by another test, which itself may not be perfect.
To understand the principles involved in assessing a screening test, let us make up a population to be screened for a particular disorder. It is represented by the upper box of Fig. 13.1, and includes 9 individuals who really have the disorder (filled squares) and who are intermingled with 31 people who are actually normal (open squares). This disorder has a prevalence of 22.5% because it occurs in 9 out of 40 people (9/40 = 0.225).
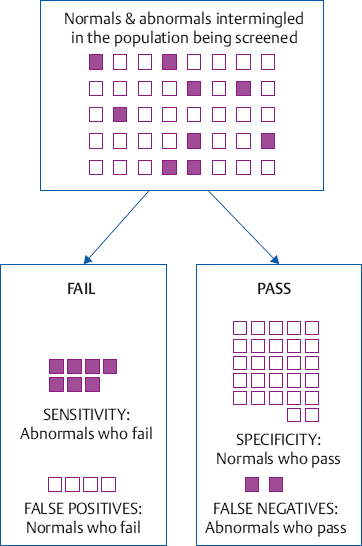
A person who passes a screening test is considered to be free of the problem, whereas one who fails is thought to have the problem. For example, a hearing screening test might involve listening for a tone. People who can hear the tone will pass the screening test, but those who cannot hear the tone will fail. Hence, on a perfect screening test, everyone who is really normal would pass and everyone who is really abnormal would fail. The results of our hypothetical screening test are represented by the two lower boxes in the figure, labeled “pass” and “fail.” Notice that the screening test outcome is not perfect: 27 of the 31 normal people passed the screening, but 4 of them failed; and 7 of the 9 abnormal individuals failed, but 2 of them passed. Hence, even though screening tests seem to have two results (pass and fail), there are really four possible outcomes from the standpoint of whether the pass and fail results are right or wrong.
The four possible outcomes of a screening test are often shown in the form of a matrix such as the one shown in Fig. 13.2. The two correct outcomes are called sensitivity and specificity. Sensitivity is the proportion of abnormal people who fail the screening test, and is also known as the hit rate. It is obtained by dividing the number of abnormals who fail by the total number of abnormals. The sensitivity of our hypothetical screening test is 7/9 = 0.78, or 78%. Fig. 13.3 shows the sensitivity and other values obtained in our hypothetical example. Specificity is the proportion of normal individuals who pass the screening test. It is calculated by dividing the number of normals who pass by the total number of normal cases, which is 27/31 = 0.87, or 87%, in our example.
The two incorrect screening outcomes are false negatives and false positives. A false-negative result, or a miss, occurs when an abnormal person passes the screening test. In contrast, a false-positive result occurs when a normal person fails. Passing the screening test is a “negative” result because it implies the person does not have the problem, and failing the screening test is a “positive” result because it suggests the person does have the problem. The false-negative rate is the proportion of abnormal cases who pass the test, that is, the number of misses divided by the total number of abnormals. For our hypothetical data the false-negative rate is 2/9 = 0.22, or 22%. The false-positive rate is the proportion of normals who fail the screening test. It is obtained by dividing the number of false positives by the total number of normals, which is 4/31 = 0.13, or 13%.
In summary, sensitivity (or the hit rate) tells us how well the screening test correctly identifies people who have the problem, and specificity shows how well the test correctly identifies those who are normal. The false-negative (miss) and false-positive rates are the errors associated with sensitivity and specificity, respectively. The goal is to have a screening test with both good sensitivity and good specificity. Even a very sensitive screening test would be useless if it is also failed by too many people who are normal, and a test with great specificity would be useless if it is also passed by too many people who are abnormal.
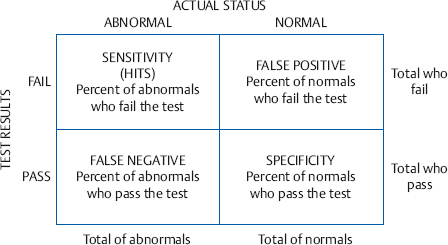
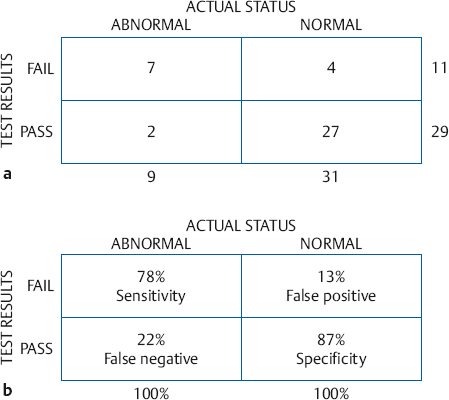
Fig. 13.3 (a) Number of patients in each category from the screening test example in Fig. 13.1. (b) Sensitivity, specificity, false-positive, and false-negative rates for this example.
 Prevalence of Hearing Impairment
Prevalence of Hearing Impairment
Newborns The need for hearing screening in infants and children becomes clear when we consider the high prevalence of hearing loss, the impact of hearing impairment, and the importance of early intervention. Prevalence estimates for infant hearing loss from the 1990s ranged from about 1 to 6 per 1000 births depending on the degree of loss and whether one or two ears were involved, rising to ~ 2 to 4% among at-risk babies like those in the neonatal intensive care unit (NICU; e.g., Mauk & Behrens 1993; Stein 1999). More recent findings place the prevalence of infants in the United States with diagnosed hearing loss among those who were screened during 2011 at 1.5 per 1000 (CDC 2013).
Children and adolescents Estimates of the prevalence of hearing loss among children, adolescents, and young adults have varied widely between roughly 3 and 33%, depending on how “hearing loss” is defined and a host of differences in methodology, sampling, and how confounding influences were addressed (e.g., Sarff 1981; Axelsson, Aniansson, & Costa 1987; Lundeen 1991; Montgomery & Fujikawa 1992; Bess, Dodd-Murphy, & Parker 1998; Niskar et al 1998; Augustsson & Engstrand 2006; Rabinowitz, Slade, Galusha, Dixon-Ernst, & Cullen 2006; Henderson, Testa, & Hartnick 2011; Schlauch & Carney 2011, 2012; Schlauch 2013).
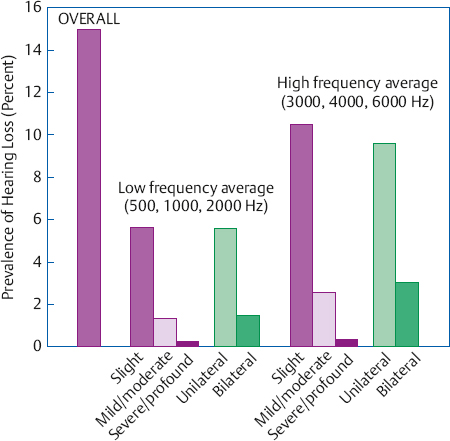
An analysis of the 1988–1994 National Health and Nutrition Examination Survey (NHANES)2 by Niskar et al (1998) and a large-sample study by Bess et al (1998) suggested that the overall prevalence among American school children is ~ 11 to 15%. Niskar et al (1998) categorized losses as slight, mild/moderate, and severe/profound based on a low-frequency average (500, 1000, 2000 Hz) and a high-frequency average (3000, 4000, 6000 Hz). Bess et al (1998) distinguished between minimal sensorineural hearing losses and other types and degrees of hearing loss (Table 13.1). Niskar et al (1998) found that slight losses (16–25 dB HL) are more prevalent than greater degrees of hearing loss (Fig. 13.4); and Bess et al (1998) found a prevalence of 5.4% for various types of minimal sensorineural hearing loss and 5.9% for other categories of hearing loss (Fig. 13.5). In addition, both studies also found high-frequency hearing losses among school-age children, although there were different prevalence rates at 3% by Bess et al (1998) and 12.7% by Niskar et al (1998).3
2 The NHANESs are available on line from the Centers for Disease Control and Prevention at www.cdc.gov/nchs/nhanes.htm.
Minimal sensorineural hearing loss (SNHL) categoriesb
| |
Bilateral minimal SNHL
|
• 500–2000 Hz pure tone-average (PTA) 20–40 dB HL in both ears
|
Unilateral minimal SNHL
|
• 500–2000 Hz PTA ≥ 20–40 dB HL in poorer ear
• 500–2000 Hz PTA ≤ 15 dB HL in better ear
|
High-frequency SNHL
|
• ≥ 2 thresholds ≥ 25 dB HL among 3000, 4000, 6000, and 8000 Hz
• One or both ears
|
Other hearing loss categoriesc
| |
Conductive hearing loss
|
• Average air conduction thresholds ≥ 25 Hz
• Average air-bone-gap ≥ 10 dB HL
• Type B tympanogram
• One or both ears
|
Other hearing loss
|
• Hearing losses not falling into the other groups (e.g., greater than minimal sensorineural losses, mixed losses)
|
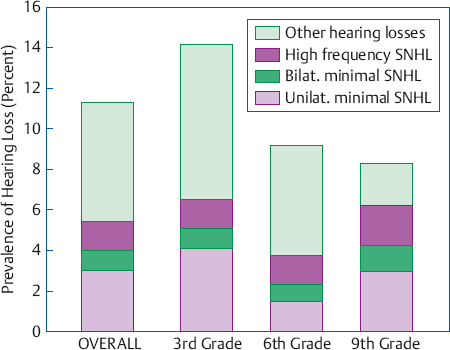
Fig. 13.5 Prevalence of hearing losses among 1218 children in the third, sixth, and ninth grades according to the categories defined in Table 13.1. (Based on Bess, Dodd-Murphy, & Parker [1998].)
A comparison of the 1988–1994 and 2005–2006 NHANES results by Shargorodsky, Curhan, Curhan, & Eavey (2010) revealed that the prevalence of hearing loss among American 12- to 19-year-olds between these two time periods rose from 14.9 to 19.5% for losses that were > 16 dB HL (slight or worse) and from 3.5 to 5.3% for losses ≥ 25 dB HL (mild or worse). Of particular importance is that the increase was more common and statistically significant for the high frequencies (12.8 to 16.4%), but less common and not significant for the low frequencies (6.1 to 9.0%). Since noise exposure is associated with high-frequency hearing loss (see Chapter 17), one compelling implication of this increase is that the impact of excessive noise exposure is growing among adolescents.
It is no surprise that the findings just described precipitated a considerable amount of media attention.4 However, subsequent analyses of the same survey data indicated that the prevalence of high-frequency hearing loss among American adolescents actually did not increase between the 1988–1994 and 2005–2006 surveys (Henderson et al 2011; Schlauch & Carney 2012). The analysis by Schlauch and Carney (2012; see also Schlauch 2013) is of particular interest because it excluded cases with any evidence of outer or middle ear disorders, and accounted for other confounds such as hearing losses involving both the low and high frequencies as opposed to just the highs. The resulting analysis revealed that the prevalence of high-frequency losses for teenagers in the 2005–2006 survey was only 7.4 to 7.9% (depending on whether 8000 Hz was included in the average), which is, of course, much more optimistic than the 12.8 to 16.4% rates calculated in the other studies (Niskar et al 1998; Shargorodsky et al 2010). In a similar vein, the prevalence of high-frequency hearing loss did not increase for 18-year-old Swedish males tested during 1969–1977 compared with those tested in 1998 (Augustsson & Engstrand 2006), or for American 17- to 25-year-olds tested between 1985 and 2004 (Rabinowitz et al 2006). This does not mean that the prevalence of high-frequency hearing loss will remain steady into the future, particularly in light of what appear to be increasing opportunities for environmental, recreational, and workplace noise exposure (see Chapter 17). On the contrary, hearing loss prevalence throughout childhood and adolescence certainly bears monitoring over time.
3 Let’s use this difference as an opportunity to illustrate why it is important to pay attention to how terms are defined and how subjects are placed into groups. The Niskar et al (1998) prevalence figures for high-frequency losses are close to those for older children and teenagers by Axelsson, Aniansson, & Costa (1987) and by Montgomery and Fujikawa (1992). However, those studies found prevalence rates of ~ 6% for 7-year-olds and second graders, whereas Niskar et al found similar percentages for 6- to 11-year-olds (12.2%) and 12- to 19-year-olds (13%). The Niskar et al 6–11-year-old age range included 7-year-olds (who had a lower prevalence in the earlier studies) and 10-year-olds (who had a high prevalence rate). Also, Bess et al (1998) commented that their prevalence rates were similar to or higher than the ones by Axelsson et al and by Montgomery and Fujikawa when they recalculated their data using the definitions of high-frequency loss from those studies. Thus, some of the discrepancies may be related to differences in how high-frequency hearing loss was defined and possibly to how the children were grouped by age. See Schlauch and Carney (2011, 2012) for additional information about confounding influences in hearing surveys and how they affect hearing loss prevalence rates.
4 For example, a Washington Post headline read, “Study shows sharp increase in hearing loss among U.S. teens, especially boys” (available at www.washingtonpost.com/wp-dyn/content/article/2010/08/17/AR2010081705861.html). The headline points out that the analysis by Shargorodsky et al (2010) revealed a larger increase in high-frequency loss for boys. Ironically, even though the analysis by Henderson et al (2011) showed no prevalence increase overall, it did reveal a prevalence increase for girls.
Adults The prevalence of hearing impairments among adults increases with age from roughly 5% among young adults to over 40% among the elderly. Fig. 13.6 illustrates this trend in terms of both self-identified hearing difficulty (Pleis, Lucas, & Ward 2009), as well as better-ear thresholds exceeding 25 dB HL for the frequencies between 500 and 4000 Hz (Mitchell, Gopinath, Wang, et al 2011).
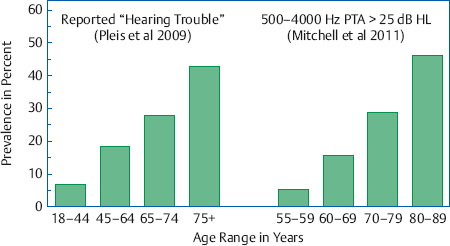
Fig. 13.6 Estimated prevalence of hearing impairments through the adult years based on those reporting “hearing trouble” in the U.S. National Health Interview Survey (left panel; Pleis et al 2009), and those in the Australian Blue Mountains Hearing Study with pure tone averages for 500, 1000, 2000, and 4000 Hz greater than 25 dB HL in the better ear (right panel; Mitchell et al [2011]).
It is heartening to note, however, that comparing the NHANES results obtained over the years shows that the hearing status of American adults appears to be better now than it was in the past. In particular, the overall prevalence of hearing loss (≥ 25 dB HL) among 25- to 69-year-old adults without diabetes fell from 27.9% during 1971–1973 to 19.1% during 1999–2004 (Cheng et al 2009); and adults’ median thresholds were better in 1999–2004 than they were in 1959–1962 (Hoffman, Dobie, Ko, Themann, & Murphy 2010).
 Audiological Screening in Infants and Children
Audiological Screening in Infants and Children
Prevalence rates like those just described make it clear that we need a strategy to identify hearing-impaired infants as early as possible and to continue screening efforts in children through the school years.
The adverse impact of hearing impairment on speech and language, literacy and academic performance, and psychosocial factors is substantial and well established (see, e.g., AAA 1997a,b; ASHA 1997; JCIH 2007; Tye-Murray 2009). Even children with minimal sensorineural hearing loss and unilateral hearing loss experience educational and psychosocial difficulties (e.g., Bess et al 1998). The key to mitigating these effects lies in early identification leading to early intervention. Particularly impressive is the finding of significantly better language skills among hearing-impaired children who were identified by the time they were 6 months old compared with those who were identified later than this (Yoshinaga-Itano, Sedey, Coulter, & Mehl 1998).
 Newborn Hearing Screening
Newborn Hearing Screening
Early hearing detection and intervention (EHDI) refers to the systematic identification of babies with hearing loss and the provision to them of comprehensive habilitative approaches as early as possible. It has been endorsed by major professional organizations, state and federal legislation, and international groups, and is the subject of extensive clinical and research efforts.5 Universal newborn hearing screening (UNHS) by 1 month of age, diagnosis by 3 months, and commencement of an intervention program by 6 months (the “1-3-6 rule”) is viewed as the goal throughout the United States (e.g., White, Vohr, Meyer, et al 2005; JCIH 2007). In fact, 98.4% of babies born in the United States6 were screened for hearing loss in 2011, with 94.9% being screened by 1 month of age (CDC 2013).
A variety of approaches and techniques for identifying hearing loss in infants have been used over the years. In the broadest terms, these include (a) public awareness campaigns, (b) high-risk registers, and (c) screening programs employing behavioral and/or physiological tests, often combined with the use of risk indicators.
Public Awareness Campaigns
The public awareness approach uses such methods as mass media campaigns, brochures, and checklists to educate the public about the danger signs of hearing loss in children. The idea is to make parents and other caregivers aware of the problem and able to identify it so they can refer the child for diagnosis and treatment. Although public awareness campaigns are a valuable adjunct to hearing loss identification in general, they are not effective by themselves because there is great uncertainty about who actually receives and responds to these efforts, and concerns that many primary care health providers might tend to discount parental suspicions (Elssmann, Matkin, & Sabo 1987; Mauk, White, Mortensen, & Behrens 1991).
High-Risk Registers
Another approach that has been used in the early identification of hearing-impaired babies involves determining whether the child meets any of several criteria associated with hearing loss. Infants identified by this high-risk register are then referred for evaluation and their cases are followed over time. Table 13.2 summarizes a contemporary list of risk indicators (JCIH 2007), although they are actually part of a comprehensive early identification program as opposed to being a stand-alone high-risk register. Hearing loss identification programs based on high-risk registers are relatively inexpensive to administer, but they were found to be subject to significant problems (e.g., Pappas 1983; Elssmann, Matkin, & Sabo 1987; Mauk et al 1991; NIH 1993): There were difficulties involved in gathering the needed information. For example, the information used to decide whether a baby should be placed on the high-risk register was usually based on birth certificate information or maternal questionnaires. Moreover, it has been shown that high-risk registers miss about half of all hearing-impaired newborns, and many children have been lost to follow-up.
5 The interested student will find up-to-date information, reference material, internet links, etc., pertaining to all aspects of newborn screening and related matters at web sites like the ones maintained by the Centers for Disease Control and Prevention (www.cdc.gov/nceh/programs/CDDH/ehdi.htm), American Speech-Language-Hearing Association (www.asha.org), American Academy of Audiology (www.audiolog.org), Joint Committee on Infant Hearing (www.jcih.org), and the National Center for Hearing Assessment and Management (www.infanthearing.org).
Table 13.2 Risk indicators for congenital, progressive, and delayed-onset hearing loss based on the JCIH (2007) position statement
Familial history of permanent hearing loss in childhood (delayed-onset risk)
|
Prenatal infections, especially
• Cytomegalovirus (delayed-onset risk)
• Herpes
• Rubella
• Toxoplasmosis
• Herpes
• Syphilis
|
Craniofacial anomalies (e.g., anomalies of pinna, external auditory meatus, temporal bone, ear pits and/or tags)
|
Syndromes involving congenital hearing loss, delayed-onset or progressive hearing loss (delayed-onset risk) Examples: Alport syndrome, Jervell syndrome, Lange-Nielson syndrome, neurofibromatosis, osteopetrosis, Pendred syndrome, Usher syndrome, Waardenburg syndrome
|
Physical characteristics associated with syndromes involving sensorineural (e.g., white forelock) or permanent conductive hearing loss
|
Neonatal intensive care exceeding 5 days
|
Neonatal intensive care of any duration involving
• Extracorporeal membrane oxygenation (delayed-onset risk)
• Assisted ventilation
• Hyperbilirubinemia with exchange transfusion
• Ototoxic drugs (e.g., gentimycin, tobramycin, loop diuretics)
|
Neurodegenerative disorders (delayed-onset risk) Examples: Charcot-Marie-Tooth syndrome, Friedreich ataxia, Hunter syndrome
|
Postnatal infections associated with sensorineural hearing loss (delayed-onset risk)
• Bacterial meningitis
• Viral meningitis (especially herpes, varicella)
|
Chemotherapy (delayed-onset risk)
|
Head trauma, especially fracture of temporal bone/skull base (delayed-onset risk)
|
Caregiver concerns (delayed-onset risk) about
• Hearing
• Speech
• Language
• Developmental delay
|
Screening Approaches
Behavioral Screening
Behavioral methods (e.g., Wedenberg 1956; Downs & Sterritt 1967) were used for infant hearing screening in the past. Recall from Chapter 12 that behavioral observation (or “behavior observation audiometry”) involves presenting a stimulus to the child and watching for changes in behavior appropriate for her stage of development. With newborns, this involves determining whether rather intense stimuli (typically 60 dB SPL or more) evoke responses such as a startle reflex, an auropalpebral reflex, or arousal from sleep. Automated approaches were also used to identify behavioral responses to high-level stimuli, such as the Crib-O-Gram (Simmons & Russ 1974), which employed a crib fitted with motion detectors that monitored the infant’s movements, and the Neonatal Auditory Response Cradle (Bennett 1975; Shepard 1983), which monitored respiratory changes as well as body movements.
Behavioral observation approaches are no longer used in neonatal screening because of several serious limitations (e.g., Northern & Gerkin 1989; Durieux-Smith & Jacobson 1985; Durieux-Smith, Picton, Edwards, Goodman, & MacMurray 1985; Shimizu et al 1990; Mauk & Behrens 1993). They involve subjective judgments that are highly susceptible to bias; there are considerable reliability problems as well as many false-positive and false-negative results; and the use of high-level stimuli presented from a loudspeaker, so that mild and moderate losses cannot be identified, and it is impossible to tell whether a response was due to hearing the sound in one or both ears. However, conditioned behavioral methods can be used with older infants and toddlers, as described below.
Physiological Screening
Physiological measures have become the standard means of testing in neonatal hearing screening programs. The principal techniques are the auditory brainstem response (ABR), the auditory steady-state responses (ASSR) and otoacoustic emissions (OAE) (e.g., NIH 1993; ASHA 1997; JCIH 2007; Gravel, White, Johnson, et al 2005; Johnson, White, Widen, et al 2005a,b; White et al 2005; Widen, Johnson, White, et al 2005); and auditory steady-state responses (ASSR) are also being used as an infant screening method (e.g., Savio, Perez-Abalo, Gaya, Hernandez, & Mijares 2006). In addition to good sensitivity and objectivity, the physiological methods can be used when the infant is sleeping, and permit us to screen each ear separately. These methods require more costly instrumentation than behavioral approaches, tend to be limited in their ability to detect low-frequency hearing losses, and reflect the integrity of the peripheral and lower auditory system rather than the notion of “hearing” that is inferred from a behavioral response.
The auditory brainstem response is well established as a neonatal hearing screening test and has impressive rates of sensitivity, specificity, and reliability (e.g., Mauk & Behrens 1993; Finitzo, Albright, & O’Neil 1998; Vohr, Carty, Moore, & Letourneau 1998; Norton, Gorga, Widen, et al 2000; Hall 2007; Sininger 2007). Successful screening outcomes have been found for both transient-evoked otoacoustic emissions (TEOAEs; e.g., Bonfils, Uziel, & Pujol 1988; Uziel & Piron 1991; Maxon, White, Behrens, & Vohr 1995; Prieve 1997; Thompson 1997; Finitzo et al 1998; Vohr et al 1998; Gravel, Berg, Bradley, et al 2000; Dalzell, Orlando, MacDonald, et al 2000; Norton et al 2000; Prieve, Dalzell, Berg, et al 2000; Prieve & Stevens 2000; Spivak, Dalzell, Berg, et al 2000) and distortion product otoacoustic emissions (DPOAEs; e.g., Bonfils, Avan, Francois, Trotoux, & Narcy 1992; Lafreniere, Smurzynski, Jung, Leonard, & Kim 1993; Brown, Sheppard, & Russell 1994; Bergman et al 1995; Norton et al 2000). The EOAE shares excellent sensitivity with the ABR for detecting hearing loss in infants, although its specificity may not be quite as high as that obtained with the auditory brainstem response. Moreover, the ABR can be used to screen for auditory neuropathy spectrum disorder, whereas the preneural nature of OAEs makes them inappropriate for this purpose (e.g., JCIH 2007). The use of OAEs as a screening tool has also been reported in preschoolers (Sideris & Glattke 2006; Eiserman et al 2007), school-age children (Nozza, Sabo, & Mandel 1997), and adults (Engdahl, Woxen, Arnesen, & Mair 1996; Scudder, Culbertson, Waldron, & Stewart 2003; Seixas et al 2005).
Universal newborn hearing screening becomes simpler, quicker, and more cost-efficient when automated auditory brainstem response (A-ABR) or otoacoustic emissions screening devices are used in place of clinical instrumentation. These instruments employ statistical criteria to determine if an acceptable response is present, leading to a “pass” versus “refer” recommendation instead of an ABR or OAE record that must be professionally interpreted. As a result, the routine aspects of carrying out the screening program do not require highly trained professionals to perform the tests. Thus, it is not surprising that automated ABR and/or OAE devices are widely used in neonatal screening programs (e.g., Jacobson, Jacobson, & Spahr 1990; Herrmann, Thornton, & Joseph 1995; Prieve 1997; Thompson 1997; Mason & Herrmann 1998; Mason, Davis, Wood, & Farnsworth 1998; Gravel et al 2005; Johnson et al 2005a,b; White et al 2005; Widen et al 2005; Uus & Bamford 2006; Lévêque, Schmidt, Leroux, et al 2007; Lin, Shu, Lee, Lin, & Lin 2007).
Numerous proposed guidelines and position statements have been published over the years in an evolutionary attempt to arrive at the optimal strategy for identifying hearing-impaired infants. Let us briefly outline some of the approaches to the issue, being mindful that (1) we are dealing with an evolutionary process in the development of strategies for the early identification of hearing impairment, and (2) no single protocol can be expected to be the best one for every screening program and setting. These caveats are not limited to hearing screening in babies; they also apply to screening approaches used for children and adults, discussed later in this chapter.
NIH Consensus Statement (1993)
A consensus statement on the early identification of hearing impairment prepared by a National Institutes of Health multidisciplinary panel (NIH 1993) calls for the universal screening for hearing impairment of all neonates regardless of whether they are at high risk or low risk for hearing impairment. This screening should occur within 3 months of birth, and preferably before the infant has been discharged from the hospital because accessibility is greatest while babies are in the newborn nursery. Recognizing that many hearing losses develop or worsen after the neonatal period, the NIH panel also recommended that surveillance for hearing impairment continue through early childhood. They also pointed out that another opportunity for universal screening presents itself when children enter school.
The newborn screening approach suggested by the NIH panel is a two-tier protocol involving TEOAE screening for all babies followed by ABR screening for those who fail the TEOAE screen. The TEOAE screening is done first because it is very sensitive to hearing loss, is fast, and does not require the use of electrodes. Neonates who pass the OAE screen are considered normal. Those who fail the OAE screening proceed to the next step (ABR screening) to minimize over-referrals (i.e., false-positive results). Babies who fail the ABR screen are referred for diagnostic evaluations. Those who pass the ABR screen are discharged, but they should be rescreened in 3 to 6 months. Although the NIH panel estimated that the two-tier TEOAE/ABR protocol is more cost-effective, it encouraged institutions that have been successfully using the ABR alone for universal newborn screening to continuing doing so.
An important multi-state study involving seven hospitals with high-quality neonatal screening programs concentrated on babies who failed the OAE but were passed by the two-tier screening protocol because they were missed by the A-ABR (Gravel et al 2005; Johnson et al 2005a,b; White et al 2005; Widen et al 2005). These babies were then seen for diagnostic evaluations when they were 8 to 12 months old. Of the 973 babies who met various selection requirements and returned for diagnosis, a PHL was found in 30 ears of 21 infants. In other words, 21 infants with PHLs failed the OAE but were passed (missed) by the two-tier screening protocol. Considering these cases along with 158 infants with PHL who failed the two-tier screen, the investigators estimated that ~ 23% of the babies with PHL were missed by the A-ABR.7 Before reacting to the 23% miss rate, we must be aware that (a) the A-ABR used a 35 dB nHL stimulus, and (b) most (71.4%) of the missed PHL cases had mild hearing losses (pure tone averages less than 40 dB HL). In contrast, most of the babies with PHL who were identified by the two-tier protocol (i.e., failed the A-ABR) had losses in the moderate-to-profound range. Certainly, fewer ears with mild hearing losses would be missed if the A-ABR used a lower screening level, such as 25 dB nHL. This is not to diminish the considerable implications of mild hearing losses. On the contrary, it highlights the need for screening programs to specify what degrees of hearing loss are being targeted for identification, and then to use techniques (e.g., screening levels) that address them. It also reveals the importance of continued surveillance of children’s hearing beyond the newborn period. Interested students should see the informative and insightful discussions of these and other considerations by Gravel et al (2005) and Johnson et al (2005a).
An important suggestion made by the NIH panel is that primary caregivers and health care providers need to be educated about hearing loss and its identification in young children. These educational efforts should highlight (1) neonatal risk factors, (2) acquired hearing impairment risk factors, (3) the early behavioral signs of hearing loss, and (4) the fact that crude “measures” of hearing ability (e.g., hand clapping) do not work and are misleading.
ASHA (1997) Infant Screening Guidelines
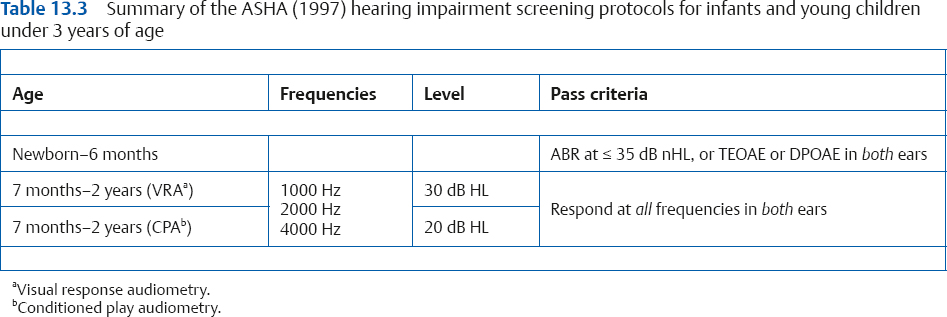
The American Speech-Language-Hearing Association (ASHA 1997) infant screening guidelines cite the JCIH goal of hearing impairment detection by 3 months old and intervention under way by 6 months of age. The ASHA guidelines call for newborns and younger infants up to 6 months of age to be screened for hearing impairment using ABR and/or otoacoustic emissions testing. The OAE test may use either transient-evoked or distortion product otoacoustic emissions. Passing the ABR test requires a response at 35 dB nHL in both ears; and passing the OAE test requires an acceptable TEOAE or DPOAE in both ears. In addition to these screening tests, the ASHA guidelines also call for surveillance based on the kinds of indicators listed in Table 13.2, which continue to be considered as the child gets older.
JCIH (2007) Infant Screening Guidelines
The Joint Committee on Infant Hearing (JCIH) has provided position statements on hearing loss identification in infants since 1982, and has revised them to reflect accumulating knowledge and scientific advances over the years. The current position statement (JCIH 2007) calls for (a) physiological hearing screening of all infants before they are 1 month old, (b) confirmation of the hearing loss before 3 months of age, and (c) commencement of an interdisciplinary intervention program before the infant is 6 months old. Moreover, the scope of disorders targeted for identification been expanded to include neural hearing loss (i.e., auditory neuropathy spectrum disorder) in addition to sensorineural (cochlear) and permanent conductive hearing losses.
In general, the JCIH protocol calls for physiological screening (and rescreening for those who fail the initial screen) before discharge from the hospital, and comprehensive diagnostic evaluations for infants who fail the screening protocol. However, different screening protocols are recommended for infants in well-baby nurseries and those in the NICU.
Neonates in the well-baby nursery may be screened using A-ABR or OAEs, and those who fail an initial screen must be prescreened before discharge with the same technology that was used initially. (Babies discharged before screening or born outside of the hospital should have an outpatient screening by 1 month of age.) Regardless of whether the initial screening is failed in one or both ears, rescreenings should always be done for both ears. Two-tier screening is permitted as long as those who fail an initial OAE screen are rescreened by A/ABR; in which case passing the A/ABR rescreen constitutes a “pass.” On the other hand, those who fail an initial A/ABR screen should not be rescreened by OAE, because passing the OAE rescreen would not change the fact that the baby has been identified as being at risk for auditory neuropathy spectrum disorder. Infants failing the rescreening are referred for comprehensive audiological evaluations.
Because babies in the NICU are considered to be at risk for auditory neuropathy spectrum disorder, they should be screened with ABR techniques. In addition, NICU babies who fail the initial screen should be rescreened by an audiologist, and have a comprehensive audiological evaluation if they fail the rescreen.8 The Guidelines Development Conference (GDC 2008) has endorsed ABR screenings for NICU babies, and added that infants in the well-baby nursery should also be screened by ABR whenever the family history includes “childhood hearing loss or sensory motor neuropathy” (GDC 2008, p. 7).
Risk indicators are used to help identify children with delayed-onset or progressive hearing losses, as well as those with mild losses, who are likely to have passed the newborn screening protocol. Table 13.2 summarizes the hearing loss risk indicators recommended by the JCIH (2007). Notice that it includes items targeting progressive and delayed-onset hearing losses as well as congenital losses. Many of the indicators are observable during or soon after birth (e.g., structural anomalies) or become apparent during the postnatal hospital stay, such as those related to care in the NICU. Some rely to a greater or lesser extent upon historical information (e.g., family history of hearing loss and, to some extent, infections during pregnancy). Others may not become apparent for quite some time, perhaps years later (e.g., head trauma, meningitis). Children with risk indicators should have at least one audiological evaluation by the time they are 30 months old, and more frequent evaluations are recommended for those with indicators for delayed-onset hearing loss.
In addition, the JCIH (2007) recommends ongoing surveillance for all children in the child’s medical home (typically the pediatrician or family practitioner) according to the pediatric periodicity schedule (AAP 2000) during regularly scheduled well-care visits; as well as the administration of a validated screening tool at 9, 18, and 24 or 30 months (AAP 2006), or sooner if there are caretaker concerns or suspicions based on the physician’s observations. The American Academy of Pediatrics calls for neonatal screening and hearing screenings in the pediatric office at certain ages up to 10 years old (AAP 2008; Harlor & Bower 2009). During these visits, attention is given to the risk indicators in Table 13.2, developmental milestones, and other factors such as persistent middle ear fluid.
Screening Babies Beyond 6 Months of Age (ASHA 1997)
There are many reasons to screen babies after the sixth month. Regardless of our goals and efforts to effect universal screening within the newborn period, there will always be at least some infants who have not been screened by the time they reach 6 months old. Other babies will require rescreening based on risk indicators (often at regular intervals), suspicions that develop over time, and various screening mandates that might apply. In fact, phrases like “as needed, requested, or mandated” appear as screening indicators throughout the guidelines.
The ASHA (1997) screening guidelines recommend that pure tone screening should be done at 1000, 2000, and 4000 Hz using conditioned response methods for children in the age range from 7 months to 2 years. The test tones should be presented at a screening level of 30 dB HL using visual reinforcement audiometry (VRA) or at 20 dB HL using conditioned play audiometry (Table 13.3). These methods require the screening to be done by audiologists rather than by support personnel. The inability to hear any tone in either ear constitutes a failure, leading to rescreening or an audiological evaluation. Sound field testing may be an acceptable modification for children who refuse earphones, keeping in mind that we do not know which ear(s) are responsible for a response to a sound field stimulus. However, unconditioned methods like behavioral observation are not considered acceptable. Of course, there will be children in this age range who cannot be reliably tested with conditioned audiometric techniques, in which case ABR and OAE should be used.
 Screening in Preschool and School-Age Children
Screening in Preschool and School-Age Children
Hearing screening through the childhood years is important because many hearing losses cannot be identified during the newborn screening processes. These are not just cases of false negative newborn screening outcomes. Many hearing losses become apparent during childhood because they are of delayed onset or progressive in nature, or are caused by such things as illness, physical trauma, noise exposure, or ototoxicity (ASHA 1997; Bamford, Fortnum, Bristow, et al 2005; JCIH 2007; Harlor & Bower 2009; AAA 2011; see also Table 13.2). Several examples of the recommended timing of routine hearing screenings are shown in Table 13.4. Two of them are from the comprehensive school hearing screening guidelines we will discuss in some detail below (ASHA 1997; AAA 2011), and the third one is recommended by the American Academy of Pediatrics as part of regular preventive pediatric health care visits for otherwise healthy children (AAP 2008; Harlor & Bower 2009). Notice that the recommended screening schedules are similar up to the first grade or ~ 6 years old, but differ afterward, especially for those during pediatric visits that do not continue after age 10.
Enter school
|
Preschool 4
|
years old
|
Kindergarten
|
Kindergarten
|
5 years old
|
First grade
|
First grade
|
6 years old
|
Second grade
| ||
Third grade
|
Third grade
|
8 years old
|
Fifth grade
|
10 years old
| |
Seventh grade
|
Seventh or ninth grade
| |
Eleventh grade
|
Before proceeding, it is wise to point out that there will be many references to otitis media with effusion (OME) and middle ear effusion (MEE). We will use these terms interchangeably here to refer to the presence of fluid in the middle ear without any signs or symptoms an infection (e.g., Stool, Berg, Berman, et al 1994; AAA 2011).
ASHA (1997) Screening Guidelines
The screening guidelines recommended by ASHA (1997) call for hearing screenings to be administered when the child enters school; annually in kindergarten (K) through the third grade; and then in grades 7 and 11. The screening protocol involves determining whether the child can hear pure tones of 1000, 2000, and 4000 Hz presented at a screening level of 20 dB HL. Each ear is tested separately by air-conduction. To pass the screen, the child must respond to all of the tones presented in both ears. Missing one or more of the tones in either ear constitutes a failure. Those failing the screening test should be rescreened during the same session. Children who fail the rescreening (or could not be conditioned for the screening test) should be referred for audiological evaluations, to be followed by the appropriate kind of management.
In addition to the regularly scheduled screenings in grades K–3, 7, and 11, additional screenings are recommended when special circumstances or risk factors exist. In particular, hearing screenings should take place are when a child
• initiates special education;
• repeats a grade;
• was absent for the last “regularly scheduled” screening; or
• enters a new school system without evidence of having passed the previous scheduled hearing screening.
The risk factors indicating the need for a hearing screen include
• concern about the child’s hearing, speech, language, or learning;
• history of delayed and/or late-onset hearing loss in the family;
• signs of syndrome that includes hearing loss;
• craniofacial and/or ear anomalies;
• persistent or recurrent otitis media with effusion;
• head trauma with unconsciousness;
• exposure to ototoxic drugs; and
• exposure to potentially harmful noise levels.
The ASHA (1997) screening guidelines also include procedures to screen for outer and middle ear disorders in children: The protocol includes (1) a case history obtained from the child’s parent or guardian; (2) otoscopic inspection for obvious structural anomalies and obstructions of the ear canal and tympanic membrane; and (3) low-frequency (220 or 226 Hz) tympanometry. Pure tone screening is not employed by contemporary protocols for identifying disorders of the outer and middle ear (ASHA 1997; AAA 1997a,b, 2011).
The child should be referred for a medical examination if any of the following conditions are identified for either ear:
• drainage from the ear (otorrhea);
• ear pain (otalgia);
• structural anomalies of the ear that were not previously identified;
• ear canal abnormalities (e.g., impacted cerumen, foreign body, blood or other secretion, atresia, stenosis, otitis external); or
• eardrum abnormalities or perforations.
A medical referral is also indicated if there is a flat tympanogram when the ear volume exceeds 1.0 cm3 (suggesting perforation of the tympanic membrane) unless the excessive volume is explained by the presence of a tympanostomy tube and/or the child has a perforation that is under medical care. The tympanograms are also evaluated in terms of static acoustic admittance (YTM in mmhos) and tympanometric width (TW, which is the pressure interval, or how wide the tympanogram is in daPa, when measured halfway down from its peak). The criteria for failure are static acoustic admittance that is too low and/or tympanometric width that is too wide. The specific failure criteria recommended by ASHA (1997) were: (1) static admittance < 0.2 mmho and/or TW > 235 daPa for infants (Roush, Bryant, Mundy, Zeisel, & Roberts 1995), and (2) static admittance < 0.3 mmho and/or TW > 200 daPa for those 1 year old through school age (Nozza, Bluestone, Kardatzke, & Bachman 1992, 1994). Screening failures on this basis should result in referral for a rescreening, and failure of the rescreening should result in a referral for a medical examination.
Table 13.5 AAA (2011) minimum screening protocol for children 3 years of age and older
Pure tone screening (all children)
| ||
Frequenciesa
|
Level
|
Failure criteria
|
1000 Hz
2000 Hz
4000 Hz
|
20 dB HL
| |
Otoacoustic emissions screening (preschool, kindergarten if pure tone screening is not feasible)
| ||
Test
|
Levels
|
Failure criteria
|
DPOAE
|
L1: 65 dB SPL
L2: 55 dB SPL
|
Does not meet appropriately chosen cutoff criteria
|
TEOAE
|
80 dB SPL
| |
Immittance screening (if failure on pure tone/OAE rescreening)
| ||
Test
|
Failure criteria
| |
Tympanometry
|
Tympanometric width ≥ 250 daPa
or
Static admittance < 0.2 mmho
or
Tympanometric peak (middle ear) pressure more negative than –200 daPac
| |
The ASHA (1997) guidelines also point out that different screening guidelines may sometimes be appropriate depending on the nature of the population being screened. For example, Nozza et al (1992, 1994) found different 5 to 95% normal ranges for the general population of children and those from a subpopulation who were at risk for middle ear effusion. Several examples of these differences are shown in Table 13.6. Thus, different pass/fail criteria may be appropriate depending on whether the children being screened are from the general (“unselected”) population or from a subgroup known (“selected”) to have a higher than average risk for middle ear effusion.
AAA (2011) Screening Guidelines
The most current childhood hearing screening guidelines were introduced by the American Academy of Audiology (AAA) in 2011. They share several features with the ASHA (1997) screening guidelines, but they are by no means identical. The AAA screening guidelines were developed to identify children with permanent sensorineural hearing losses and/or persistent otitis media with effusion during the preschool and school years. An overview of the AAA screening protocol is illustrated as a flowchart in Fig. 13.7. We will discuss the details of each component later.
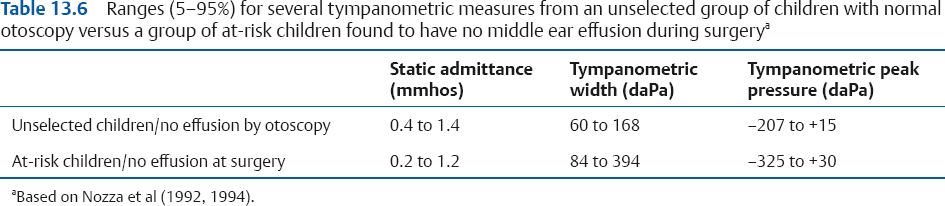
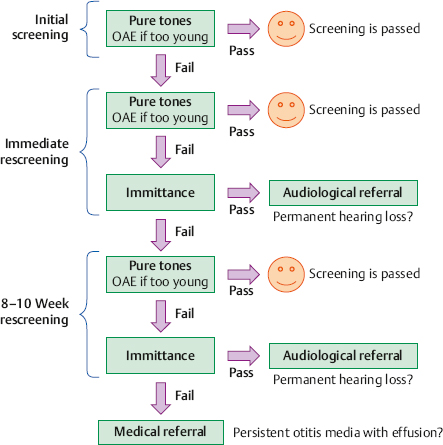
Fig. 13.7 The AAA (2011) screening protocol includes an initial screening, an immediate rescreening, and a second-tier rescreening 8 to 10 weeks later. Notice that the immittance component is a second-level procedure that is administered after failing pure tone rescreenings.

Comments
Post a Comment