ALTERNATE BINAURAL LOUDNESS BALANCE TEST(ABLB)
This
technique was initially described by Fowler, 1986, but corresponding
modifications were proposed by Hood & Jerger in new course. Currently
Fowler’s ABLB is the most preferred and commonly used procedure with Hood &
Jerger modifications whereas, the technique or MLB was described by Rager 1936,
which is helpful in detecting the recruitment in clients with bilateral hearing
loss. ABLB compares loudness growth between 2 different frequencies in the same
ear. ABLB is a pure tone test which is done when there is a threshold
difference of more than 20 dB between ears at the test frequencies and the
better ear is relatively normal.
The
purpose of ABLB test is to compare the growth of loudness in an impaired ear
with the normal growth of loudness in the opposite / normal ear.
Test approach
- Jerger protocol: In this protocol devised by Jerger tone alters between two ears every 500 milliseconds, with fixed level in abnormal ear and variable signal in the normal ear. Patient changes the intensity of the tone of variable ear until it sounds equal in loudness to the tone in the fixed ear. The tone alternates between two ears every 500 milliseconds. The tone will be off for 500 milliseconds in each ear. This off time ensures that the test tones will not be subject to adaptation.
- Hood's protocol: This protocol uses the good ear as fixed level ear and the bad ear as variable one. This protocol ensures better control by the tester.
- Miskolczy - Fodor modification: In this protocol the level of tone in fixed ear increases over time, so this ear may be considered as the reference ear. The patient uses a Bekesy tracking method to keep the level in the variable ear equally loud as the one in the reference ear. The results are automatically plotted on paper.
PROCEDURE
For
the administration of ABLB test, there is a need of 2 or dual channel audiometer
with capability of alternatively pulsing 2 tones of identical frequency from
one ear to other. The intensity of each tone must be individually controlled
from a separate hearing level dial.
The
intensity is held constant in one ear while it is varied in other ear until the
listener judges both signals to be of equal loudness. The ear with constant or
fixed intensity is termed as Reference ear and the ear with
variable intensity is termed asVariable ear. The intensity levels
in the variable ear are matched with that of loudness levels of reference ear.
The
client is instructed to state whether the variable tone is “softer than”,
“louder than” or “equal” in loudness to the reference ear. The client is
instructed that he/she will hear 2 tones, one constant in loudness and other
variable.
Judgement
of loudness is to be made only from the variable tone to the reference tone;
also the client should be cautioned to pay attention only to the loudness
changes and to ignore other differences. This is required because in case of
ABLB and MLB, where the same tone is presented in each ear, may sound different
because of the phenomenon called Diplacusis.
Carber,
1978, stated 4 variables which need to be considered while administering ABLB
technique:
I) Psychophysical method: Method limits v/s
Method of adjustment: The clinician controls both the reference and
variable ear intensity settings whereas the clinician sets the level in
reference ear while client control the variable tone intensity. Hood 1969,
supports methods of limit whereas Jerger 1962, recommends method of adjustment.
According to him, when the control of stimulus is in the client’s hand then it
has advantage of reducing the potential biases by the clinician.
II) Reference v/c variable ear: this is the most
argued option amongst clinician. Cols & others, 1974, respected Jerger’s
suggestion of using poorer ear as the reference ear, whereas, Hood, 1961,
followed Fowler’s suggestion of using the good or the better ear as the
reference ear. According to Hood, using the better ear as reference ear would
result in less variability in responses from the client as the poor being
recruiting ear will be more sensitive to changes In intensity. Jerger, 1962, stated
that if the clinician is interested in detection of presence or absence of
recruitment in poorer ear, then a few fixed settings in the poorer ear are
sufficient enough to achieve the desirable result, but if the clinician
interest is in plotting of loudness growth function as well as the
determination of presence or absence of recruitment in the poorer ear then the
Fowler’s procedure is more appropriate.
III) Number of Loudness
Balance Levels: to some degree the number of loudness balance level are
related to the following:
o Which
ear is the reference ear
o What
is the basic rationale of the test i.e. whether the aim of the search for
recruitment or the determination of loudness growth function is the desired
goal.
According
to Jerger, when poorer ear is used as reference ear then minimum 2 and maximum
3 levels are sufficient to find out recruitment, this will save time of the
clinician.
According
to Jerger, the use of good ear as reference ear would not only require more
levels of determination of the presence or absence of recruitment but would
also result in time consumption. The number of sound levels required, are more
in number when good ear is the reference ear.
According
to Fowler, more number of levels permits diagnostic judgment as well as
determination of accurate loudness growth function.
IV) Duty cycle and Alternation
rate: Jerger, 1962, recommended a tone alternation rate of 1 per
second with a duty cycle of 500msec ON and OFF per ear (i.e. the tone is ON
half the time in one ear and half the time in other ear)
Majority
of diagnostic audiometers works on these parameters though maximum clinicians
are satisfied with such settings but Hood 1969, stated that this may lead to
adaptation, hence he suggested that a duty cycle of 600msec as a better option.
However, this is not possible for the manufacturer to provide such alteration;
hence maximum clinical audiometer has a duty cycle of 500msec per ear.
PLOTTING
OF RESULTS AND INTERPRETATION:
2
primary methods have been practiced in plotting loudness balance results:
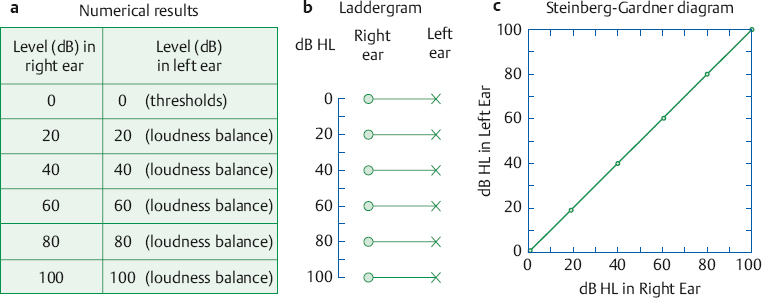
1. LADDER GRAM: Plotting on pure tone
audiogram and concept is given by Jerger. In ladder gram, equal loudness
judgment between 2 cases is connected by a straight line, the presence or
absence of recruitment is judged by inspection of the line pattern.
II) Steinberg Gardner plot: Here the values are plotted along X and Y axis as shown in the figure below.

2. GRAPHICAL FORMANT: this method is commonly known
as Fowler plot. Here the graphs are plotted of the same data as the ladder
gram. The good ear is plotted on X-axis and poorer ear is plotted on Y-axis.
The 45 degree diagonal represents idealized results for loudness balance
judgment between 2 normal ears. Comparison of lines connecting the equal
loudness points to the idealized function determines presence or absence of
recruitment.
Jerger
1962 suggested 4 results are possible:
1. COMPLETE RECRUITMENT: is present when reference and
variable ears are judged equally loud at equal HL + 10 dB.

2. If the equal loudness judgments
are made at equal SL + 10 dB, then NO RECRUITMENT is
present.

3. PARTIAL RECRUITMENT: is seen if equal loudness
judgment falls off between those of complete or no recruitment. At the highest
intensity level, equal loudness is just at 85 dBHL in good ear and 100 dBHL in
poor ear.
4. The phenomenon of DECRUITMENT is
seen less frequently than other patterns. In this case, the poorer ear needs an
ever increasing amount of intensity for a signal to sound equally loud to the
good ear. One should suspect decruitment when loudness judgment shows a SL
difference of 50 dB or more in the poorer ear than in the better ear, which is
seen in case of RCP.

4. Hyperrecruitment: Patients with Meniere's disease may exhibit a special case of recruitment in which the loudness in the abnormal ear not only catches up with the normal, but actually overtakes it. This is revealed in the laddergram by rungs that first flatten and then reverses its direction.
5. Derecruitment:
Loudness grows at a slower than normal rate as intensity increases in the abnormal ear.
Since ABLB test compares one ear with that of the other, a patient with normal and equal hearing in both ears should have:
| dB right | dB left |
| 0 | 0 |
| 20 | 20 |
| 40 | 40 |
| 60 | 60 |
| 80 | 80 |
| 100 | 100 |
Diagnostic Accuracy of the ABLB
We can consider the ABLB from the standpoint of how well it distinguishes between cochlear disorders (where there should be recruitment) and retrocochlear pathologies (where there should be no recruitment or decruitment). The ABLB has been found to identify the correct site of lesion in ~ 90% of cases for cochlear disorders and only ~ 59% for retrocochlear pathologies across studies (Turner et al 1984). These figures show that many acoustic tumor cases are misclassified as cochlear on the basis of having positive recruitment. It is possible that some retrocochlear cases might have recruitment or other characteristics of cochlear disorders (e.g., high SISI scores; see below) because of secondary damage to the cochlea (Dix & Hallpike 1958; Benitez, Lopez- Rios, & Novon 1967; Perez de Moura 1967; Buus, Florentine, & Redden 1982a).
The basic concept involves these two steps:
(1) the tumor damages the cochlea by putting pressure on its blood supply and/or adversely altering the chemistry of the cochlear fluids; and
(2) the resulting cochlear disorder then produces positive recruitment. Also, there may well be a coexisting cochlear disorder having nothing to do with retro-cochlear pathology.
For example, a patient with an acoustic tumor may well have a noise-induced cochlear impairment. These points apply to the results of other site-of-lesion tests as well.

Comments
Post a Comment